
Diagnosing PML can be challenging because the symptoms can be like those of other neurological diseases. Additionally, PML is a rare disease, so it may not be considered as a potential diagnosis initially. Improved education and awareness among healthcare professionals and patients are crucial for early detection and effective management of this challenging condition.
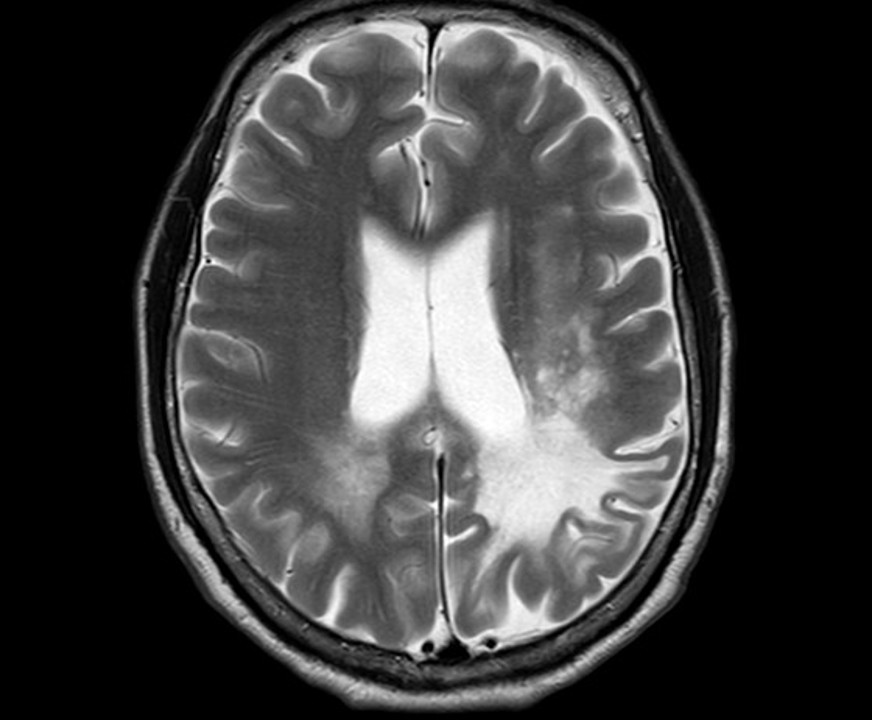
To diagnose PML, doctors typically start by taking a thorough medical history and performing a physical exam. Physicians may use various diagnostic assessments, the most important being magnetic resonance imaging (MRI) scans and cerebrospinal fluid (CSF) analysis for JC virus DNA detection. In most of the cases the diagnosis of PML is achieved in the presence of a suggestive clinical history, for example the presence of a condition of immune deficiency and the subacute onset of neurological problems together with suggestive brain lesions at MRI, and it is confirmed by the evidence of JCV DNA in the CSF.
Usually, a brain biopsy is not necessary to confirm the diagnosis. This involves removing a small piece of brain tissue and examining it under a microscope for signs of the JC virus. However, brain biopsy is an invasive procedure and carries some risks, so it is only recommended in certain situations.
Anyone with a diagnosis of PML should immediately have their physician contact a reference center for PML in her/his own country, to receive the most accurate and updated information for standard and possibly supplemental experimental treatment approaches.
Once a diagnosis of PML is confirmed, the next steps depend on the individual patient’s symptoms and overall health. There are no known interventions that can adequately treat PML if it occurs. However, the reduction of an underlying immune deficiency, when possible, may help slow or halt the progression of the disease.
If PML is associated with certain medications, it is likely that your doctor will have to discontinue the use of these medications to help restore the immune system. For patients with HIV, doctors may begin treatment with highly active anti-retroviral therapy. In some patients, particularly those with HIV and MS, it is possible that restoration of the immune system may cause an additional condition called immune re-constitution inflammatory syndrome (IRIS), which may itself lead to a decline in your condition and may lead to death or severe disability if not promptly recognized. If your doctor detects this, he or she will likely treat the inflammation inside your body.
In many cases, however, reduction of immune suppression cannot be possible, for instance on persons with congenital or other immune deficiencies, for example in the case of idiopathic CD4 cell lymphopenia, or ICL.
Apart from reduction of immune suppression, the treatment options for PML are limited, and there is no one-size-fits-all approach. Some drugs that were though to directly inhibit the capacity of JC virus to replicate in the brain cells have been used in the past and some are still used in PML patients, based on the report of anecdotical success in individual cases: these include, among the others, mirtazapine (an antidepressant drug), mefloquine (an antimalarial drug), or cidofovir (an antiviral drug active against several other viruses). None of these drugs, however, is currently recommended for treatment of PML because there is no evidence in large studies and in the clinical practice that they may help mitigate or halt the disease. It is important to know that there are recommendations against the use of some drugs, like cidofovir, whose toxic effects may be unacceptable.
In some cases, patients may also be candidate to receive experimental immune therapies to help boost the body’s ability to fight the virus. Usually, patients are referred to reference centers that have some experience with such treatments. Current experimental options are represented by the infusion of cells obtained from a donor that have been stimulated to recognize the virus (also called “viral specific T-cells”), or by the administration of “cytokines” (molecules produced by human cells that regulate the immune processes), like interleukin-7, or of immune-check-point inhibitors (molecules used for treatment of several cancers that may make human lymphocytes more active against infections). However, there is currently no evidence that they could impact significantly on the outcome of PML.
The prognosis for PML varies widely depending on the individual patient’s symptoms, overall health, and the response following reduction of immune suppression. Some patients may experience only mild symptoms and recover fully, while others may experience severe disability or even death. Some patients may experience a gradual decline in their physical and cognitive abilities, while others may experience more rapid progression of the disease. Also, although restoring the immune system may help in recovering from some PML symptoms, some of the serious effects of the disease are often permanent.